

Bullet and Splinter Wound Care Page Menu: 1 2 3 4 5 6 7 8 9 10 Next>>
Bullet and Splinter Wound Care in the Golden Age of Piracy, Page 6
Step 2F: Keep Bullet and Splinter Wounds Open
Once Step 1 of simple wound care was completed in caring for bullet wounds (Remove foreign objects), additional care was required in the deep wounds left by gunshot and large splinters. Because such wounds were required to be kept open, different procedures had to be performed which replaced steps 2 and 3 of simple wound care ('Bring the wound lips together' and 'Keep the wound lips together'). As a result, this will be referred to as Step 2F: Keep Bullet and Splinter Wounds Open. There were a variety of reasons for keeping these wounds open which primarily revolved around preparing the wound for incarning, or generating new flesh to fill these deep wounds.
Dressing a Thigh Wound, From l'Arcenal de Chirurgery,
By Johannes Scultetus, Frontispiece (1672)
To keep wounds open while they performed the needed procedures, surgeons often used tents - pieces of rolled and folded lint - which were inserted into wounds.
While they were kept open, pus and other fluid discharge from the wound had to be relieved. This was an important step in healing such deep wounds because corrupt humors - bodily fluids - had to be allowed free passage from the wound site to enable healing. In particularly deep wounds, drains were sometimes created using dressings using bandages and/or metal tubes to allow unwanted liquids to flow from the bottom of the wound.
A variety of medicines were employed during the dressing phase of bullet and splinter wound healing. These served different functions in gunshot and large splinter wounds, many of which revolved around the formation and relieving of pus which was seen as the gathering and removal of corrupted humors. Making sure medicines penetrated to the bottom of deep wounds could be challenging, with surgeons relying on tents or forcible injection by syringe.
Naturally, wounds which were being intentionally kept opened also required careful dressing if the surgeon was to keep them from becoming infected. Let's look more closely at how these things were done when dressing open bullet and splinter wounds.
Step 2F: Keep Bullet and Splinter Wounds Open - Reasons to Keep Wounds Open
From Elementarwerke fur die Jugend und Ihre Freunde, p. 37 (1774)
Military surgeon Richard Wiseman said that a wound "which is fretted and torn must also be reduced [restored] to the whole, or cut off, before your ordinary intention of Incarning [generating new flesh in the wound]."1 Wiseman was referring to repairing or removing the damaged skin at the edge of the wound.
Sea surgeon John Woodall similarly suggested that when "the outward parts about the wound be altered in colour, or grow either stinking or insensible, make scarification and foment well with strong hot Lixivium [lye]; and inject thereof into the wound very hot"2. Woodall's goal in using lye here was to make use of its cleansing and, more particularly, mollifying or softening properties in an effort to repair the damaged skin at the edge of the wound.
Thinking along similar lines, sea surgeon John Atkins explained that, in such wounds,
the Extinction of Heat is owing to the Greatness of the Contusion, (as the Ball or Splinter came with greater or less Force, direct or aslant,) and are sometimes to a great Depth, calling for Scarification and Cataplasms, to help forward the Separation of the Eschars [hardened crusts or scabs].3
The eschar referred to here is basically the same thing as the damaged skin at the edge of the wound that was discussed in the previous paragraphs.
French surgeon Ambroise Paré warned that a wound with such an eschar cannot be healed properly, because "an eschar will hinder suppuration [the formation and release of pus], which is to be desired in this kind of Wound"4. He goes on to explain that "when an Eschar is drawn, as a bar 
Photo: CDC - Wound With Eschar
over it [the gunshot or splinter wound], ...then the excrementitious [foul] humor remains longer in the part, and the putredeinous vapours hindred from passing forth, are increased, and carried from the lesser vessels to the bigger, and so over all the body."5 Here we see the problem that surgeons identified with humors being gathered at a wound site on full display. Paré is worried that unless the eschar is eliminated, the humors will have no where else to go and so will eventually remain trapped and infect the whole body.
Wiseman recommends that gunshot wounds be cured using soothing medicines which cause them to "digest [break down the eschar], separate their Sloughs [dead outer skin], and incarn [form tissue inside the wound]. But they are slow in Digestion, and require good Fomentations [poultices] and Embrocations [lotions] to cherish the native heat, which is much weakened by so great a loss of Substance."6
Although several surgeons commented on how little gunshot wounds bled in the period right after the wound occurred, Wiseman said that it could occur in the days following after the "separation of the Eschar... [W]hen you least think on it, they [veins and arteries previously damaged by the bullet] may burst out violently."7 With this in mind, he warns against putting too many compresses (dossils) into bleeding wounds, suggesting that they can cause gangrene. "Too many Instances may be given hereof: Therefore I rather advise you to us an actual Cautery."8 Wiseman is one of the few surgeons to recommend cauterization of bleeding wounds here.
Paré noted that gunshot wounds caused 'contusion and attrition', as did large splinters. He stated that "no contusion can be cured without suppuration
Photo: US Marine Corp
Simulated Suppurating Bullet Wound to the Cheek, not only according to the opinion of Hippocrates, but also of Galen and all others who have written of Physick."9 With this in mind, Richard Wiseman notes in one of his case studies that on the third day of treating the wound he "drest it up quick with my Suppuratives hot, and an Emplaster"10.
According to German surgeon Matthias Gottfried Purmann, "Some Authors are of the opinion that these Wounds may be cured without Suppuration, but if those Writers had known that Wounds made by Gun-shot cannot be cured without a Separation of the Contused Flesh, they would not talk so wildly or prescribe Impossibilities"11.
Paré warned that such wounds were slower to suppurate than simple wounds, due to the effects of "the bullet, as also the air which it violently carries before it, by much bruising the flesh, on every side, dissipates the native heat, and exhausts the spirits of the part."12 He advised that "most usually pus or quitture appears within three of four days, sooner and later according to the various complexion, and temperament of the Patients bodies, and the condition of the ambient air in heat and cold."13
His concern for the patient's 'temperament' refers to the type of body the patient had, which is connected to humor theory. Just as there were thought to be four bodily humors or fluids, it was believed that there were four basic body types, with one of the four humors being found in excess in each type.
Richard Wiseman said that the formation of pus took longer than Paré's three or four days. Wiseman recommends continuing to dress the wound so that it suppurates "to the seventh or ninth day, until you have separated the Sloughs, digested the Wound, and have a laudable Pus, (as you are wont to call it.) which is ...a perfect white Matter, of good consistence, and not fœtid or ill scented."14 Other surgeons waited even longer for suppuration to finish. In one of his case studies, John Atkins waited fourteen days for 'laudible' pus to be fully expunged from a gunshot wound!15
1 Richard Wiseman, Several Chirurgicall Treatises, 1686, p. 409; 2 John Woodall, the surgions mate, 1617, p. 143; 3 John Atkins, The Navy Surgeon, 1742, p. 150; 4,5 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 318; 6 Wiseman, p. 428; 7,8 Wiseman, p. 409; 9 Paré, p. 324; 10 Wiseman, p. 427; 11 Matthias Gottfried Purmann, Churgia Curiosa, 1706, p. 186; 12,13 Paré, p. 319; 14 Wiseman, p. 415; 15 Atkins, p. 140
Step 2F: Keep Bullet and Splinter Wounds Open - Dressing Wounds With Tents
Tents were pieces of rolled or folded material, often lint, which were placed into a wound to keep it open. This was one way to make sure medicines penetrated to the depths of such wounds as well as permitting the egress of undesirable fluids from the bottom of the wound. They had particular significance in bullet wounds, although they were also employed in deep splinter wounds as well.

Photo: J.P. Barrass - Keeping a Wound of the Hand
Open to Heal From the Bottom Up
Richard Wiseman recommended that surgeons dress bullet wounds "lightly with a proportionable soft Tent, and Pledgits dipt in some of these Digestives very warm, but not to scald them."1 Pledgits were similar to tents in that they were small pieces of lint placed into a wound. French surgeon Ambroise Paré likewise advised using tents or 'pledgets' with a complex ointment "dissolved in Venegar or aqua vitæ" added to them before insertion to resist putrefaction or rotting of the skin.2
Some period surgeons explain the use of tents in terms of keeping a wound open. Paré says that "tents are used both to keep open a Wound so long, untill all the strange bodies be taken forth, as also to carry the medicins, wherewithal they are anointed: even to the bottom of the Wound."3 He elsewhere recommends the surgeon "press a linnen boulster to the bottom of the Wound, that so the parts themselves may be mutually condensed by that pressure and the quitture [pus and other fluids] thrust forth"4.
Suggestions about the makeup of these tents for these wounds vary. Ambroise Paré says that the "tents which shall be used at the first dressing must be somewhat long and thick"5. He is particularly vocal on this point. going on to explain that large tents are useful, for "by dilating the Wound, they may make way for application of other remedies"6
Lint Tents, from A General System of Surgery by Lorenz Heister,
Plate 2, p. 20 (1750)
German surgeon Matthias Gottfried Purmann counsels that a "Tent must be made of nothing but Lint, proportioned to the Bigness of the Wound"7.
Sea surgeon John Moyle suggests placing tents in bullet wounds while the patient is in the same position in which he was shot to make sure the pathway to the bottom of the wound is straight. He tells the surgeon that the tent should "be so long as to reach almost to the bottom of the Wound, that the Medicines may touch any Vessel that is divided or wounded by [along] the way."8
When dressing a bullet wound to the shoulder, sea surgeon Hugh Ryder takes a slightly different approach, explaining that he "clapt into the Wound above the Scapula, a short thick Tent of dry Tow"9. This small tent was apparently effective as Ryder says that patient was cured in about three weeks.
Once the wound began to discharge pus or other fluids, Paré advises the surgeon to use tents which "are neither too long, nor thick, lest they hinder the evacuation of the quitture and vapours, whence the wounded part will be troubled with erosion, pain, defluxion, inflammation, abscess, [and] putrefaction"10.
Wherefore you shall put into the Wound no tents, unless small ones, and of an indifferent consistence; lest (as I said) you hinder the passing forth of the matter, or by their hard pressing of the part, cause pain, and so draw on malign symptomes.11
Purmann agrees with reducing the size of the tents, recommending that "as it [the gunshot wound] begins to mend, make your Tents lesser and lesser"12.
Artist: Adriaen Brouwer - Feeling (1635)
John Moyle uses the tent as an indicator of wound healing. "You may know when the Wound incarns by a red speck that will be at the point of your Tent when you take it out, and then must your Tents be made shorter."13
In one of his case studies John Atkins recommends the opposite treatment. He explains in one of his case studies that on the fourteenth day of healing, "a Digestion appearing on the Tent [like Moyle's 'red speck'], I rather lengthened it, and sprinkled the upper Part (as often as wanted) with an Escharotick [medicine to encourage the formation of a eshcar], to prevent the Orifice contracting too fast, and for laying a Foundation of incarning from the Bottom"14.
Atkins appears to be using medicine to encourage the upper part of the wound to form a scar on the inside so that it will not agglutinate (grow together) before the deeper parts of the wound heal. As lower parts of the wound healed, he began "shortening the Tent gradually; and at the End of a Month or five Weeks, threw it quite out and healed."15
When a bullet has gone cleanly through the body and exited, surgeons advised placing tents at both the entry and exit wound sites. Purmann explains that when "it be a through Wound, and you have an Orifice on both sides, put a Tent into each opening, but not so long as to reach one another in the middle, for you must always give this sort of Wounds sufficient Vent"16. John Moyle concurs, stating that "if the Shot went quite through, or [if it has been] cut out on the contrary side, then the Tent is [to be put] at both Orifices, and dip your double bolster in Acetum [vinegar]"17.

Artist: William Hogarth - Doctors Debating Treatment (1730)
When dealing with two such 'through' wounds, Hugh Ryder pulled "Flammulaes [small, warmed pieces] of Tow [inexpensive linen cloth] through, armed with a digestive [a medicine to encourage formation of healthy flesh], and afterward I used a short Tent to each of the four Orifices, suffering the Wounds to Incarne [form tissue] in the middle"18. Once the middle of the wound had healed, Ryder replaced the tents with smaller, medicated pledgits. When they became too large for the healing wound, he used dry pieces of lint. Unlike many of the other surgeons during this time, Ryder does not mention suppuration in these wounds to eject the undesirable humors, instead proceeding directly to healing the wound.
While Paré is in favor of using tents to keep wounds open, he also sees a need for balance so that the patient may have some measure of comfort while they are in use. "Many also offend in the too frequent use of Tents; for as they change them every houre, they touch the sides of the Wound, cause pain, and renew other malign symptomes"19. In a similar comment, John Moyle warned "you are not in this Wound, nor in any other Wounds of the Joynts, or among the Bones, to apply hard Tents, for in so doing you will but increase pain, and cause Fistulation."20
1 Richard Wiseman, Several Chirurgicall Treatises, 1686, p. 413; 2,3 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 318; 4 Paré, p. 320; 5 Paré, p. 318; 6 Paré, p. 319; 7 Matthias Gottfried Purmann, Churgia Curiosa, 1706, p. 185; 8 John Moyle, The Sea Chirurgeon, 1693, p. 74; 9 Hugh Ryder, New Practical Observations in Surgery Containing Divers Remarkable Cases and Cures, 1685, p. 82-3; 10,11 Paré, p. 319; 12 Purmann, p. 185; 13 Moyle, p. 76; 14 John Atkins, The Navy Surgeon, 1742, p. 140-1; 15 Atkins, p. 141; 16 Purmann, p. 185; 17 Moyle, p. 74-5; 18 Ryder, p. 81; 19 Paré, p. 320; 20 Moyle, p. 70
Step 2F: Keep Bullet and Splinter Wounds Open - Putting Drains in Wounds
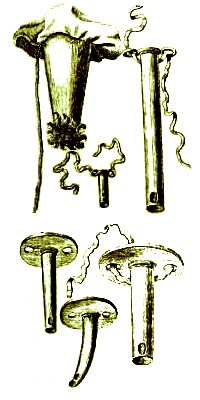
A Variety of Surgical Drains, from
A General System of Surgery
by
Lorenz Heister,
Plate 2, p. 20 (1750)
When wounds were suppurated - intentionally allowed to form pus - they naturally had to be kept open to allow the pus to escape. As Matthias Gottfried Purmann observes, "you must always give this sort of Wounds sufficient Vent. that they may sooner and better come to Suppuration."1 In addition to pus, other fluids in such deep wounds - including blood from broken vessels - needed free egress, so drains - open-ended tubes made either of bandages or metal - were sometimes placed and left in these wounds.
Some fashioned the cloth pieces they inserted into wounds so that they could function both as a tent and a drain. In a case study involving a man with a gunshot wound to the arm with a fracture, Richard Wiseman explained that he put "into the Wound only a Dossil or Tent made upon a Skewer [round wood or metal pin] soft and hollow"2. Purmann likewise says that a hollow tent could be fashioned and placed in gunshot wounds so that "the Matter and Corruption, of which these Wounds breed abundance, may have Liberty to issue out"3.
Metal tubes are also hinted at. Paré advises the surgeon to take "speciall care that the orifices of the ulcers should be kept open with hollow Tents or pipes put therein"4. He usually uses the terms 'pipe' and 'hollow bandage' interchangeably when referring to drains. While discussing the need to allow 'quitture' or discharge from a wound, Ambroise Paré elsewhere explains that it would not "be amiss to let this boulster [placed into a wound] have a large hole fitted to the orifice of the Wound and end of the hollow tent and pipe, that so you may apply a spunge for to receive the quitture, for so the matter will be more speedily evacuated and spent"5. He notes that this is particularly important when the an 'expulsive ligature' dressing is used. Such a dressing pushes humors away from and out of the wound.
1 Matthias Gottfried Purmann, Churgia Curiosa, 1706, p. 186; 2 Richard Wiseman, Several Chirurgicall Treatises, 1686, p. 427; 3 Purmann, p. 185; 4 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 323; 5 Paré, p. 320
Bullet and Splinter Wound Care Page Menu: 1 2 3 4 5 6 7 8 9 10 Next>>
Main Page • Tools & Procedures • Miscellanea • About the Author • Facebook Page
All original content copyright M. Kehoe • 2003-