

Head Surgery Page Menu: 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Next>>
Head Surgery During the Golden Age of Piracy, Page 2
Symptoms of Skull Fractures

Artist: Jonas Arnold Delineavi
Head Wound, From Armamentarium Chirurgicum Bipartitum,
by Johannes Scultetus (1666)
The most obvious sign of a skull fracture was wounding and/or irregularity of the skull. As sea surgeon John Atkins so bluntly put it, fractures can be "evident to Sense, when the largeness of the Wound makes the Fracture visible, or is sufficient for a Discovery by a Finger or Probe, or when without a Wound, the Depression is plainly felt."1
Another physical indication of such damage was swelling and similar physical changes to the area of a head wound. Sea surgeon John Moyle mentions a patient with a wound in the skull which had "grown exceeding bad, tumified [swollen] and putrified [giving off a fetid smell] at the Bone" and the man's "Head felt under the Calva [scalp] as a Quag [marshy, boggy place]".2
People who had been hit in the head sometimes showed no sign of damage to the skull, although something had clearly gone wrong. Surgical writers from this period in history often identified symptoms which indicated that a head wound was more serious than it appeared. Atkins referred to such symptoms as "Deductions from Reason, [which] are taken (when the Scalp is entire, and those Demonstrations of Sight and Touch wanting) from a Comparison between the Circumstances of receiving the Hurt, and the Symptoms conjunctly."3
Most of the period surgeons agreed that certain symptoms follow a blow to the head were indicative of a fractured skull or brain trauma.

From William Kidd and Others
of the
Pirates or Buccaneers, p. 270 (1834)
One symptom mentioned by all the period surgical authors who discussed such symptoms was impaired response from the patient. Military surgeon Ambroise Paré advised that when "the patient fall downe with the stroake, if he lye senselesse, as it were asleepe, [or] if he voyde his excrements unwittingly... you may understand that the scull is fractured, or pearced through, by the defect in his understanding and discourse."4
Surgeon Richard Wiseman noted that a man "deprived of his Speech and [use of his] Lims" required trepanning despite the lack of a 'fissure' in his cranium.5 He also mentioned "Stupor, Paralysis, &c" as symptoms of damage to the skull.6
Each of the three sea surgeons from this time period who discussed wounds of the skull in detail in their books mention impaired responses from the patient. John Woodall explained that "dull understanding, with alteration of favour and countenance do ensue; stupiditie also and dumnesse signifie the braine contused" as well as listing "dolour ....or deprivation of the functions of the senses" as symptoms.7 John Moyle said 'langour' was a symptom of severe damage to the brain and skull8. John Atkins indicated that when a "Patient also lies Senseless, Stupid and Speechless"9 after a head wound, a fractured cranium was likely.
Atkins further warned that when "a Dulness of Memory and Understanding, or a Coma"10 occurs, it was a very bad sign for the patient's recovery. Ambroise Paré likewise explained "that death is at hand if his reason and understanding faile him, if he be speechlesse, if his sight forsake him, if he would tumble headlong out of his bed, being not at all able to move the other parts of his body"11.
Artist: Gustav Dore - From The Inferno, Canto 33 (1857)
Another, sign of brain trauma was an irrationally excited or manic patient. Among his signs of skull fracture, Paré listed a patient who was "taken with giddinesse ...[and] if he have an apoplexie [unconscious, often due to stroke], phrensie, convulsion or palsie [shaking] with an involuntary excretion"12. John Moyle advised "Raving likewise is a true sign of a fractured Skull, and a contused Brain."13 Atkins listed "Deliriums, Convulsions, or a Palsy" as signs of a fracture that presaged death.14 In one of his case studies, Moyle succinctly points to this symptom. "Howbeit, by the greatness of the Blow, and astonishment of the Man, it was reasonable to suspect all was not well within."15
Fevers following a head wound were considered another possible sign of a fractured cranium. Richard Wiseman noted that a patient with no wound following a blow to the head who displayed impaired responses while under his care "was in a Feaver"16. Ambroise Paré notes that when a patient "have a continuall feaver" it is a bad sign.17 Sea surgeons John Woodall and John Atkins similarly list fever as a symptom of a contused brain.18
Bleeding was another manifestation of traumatic brain injury. Paré advised that, among other symptoms, "if blood come out at his eares, mouth, and nose... you may understand that the scull is fractured, or pearced through"19. John Moyle told his readers "your true knowledge of this thing lyes in these signs: There will be bleeding at the Mouth or Ears"20. In one of his case studies, Moyle firmly made this point; "There was Bleeding at the Ears, Eyes, Nose and Mouth... sensible Signs of a Collision of the Brain, or a Læsion of the Meninges."21 John Atkins similarly identified "Bleeding at the Nose or Ears" as one of his symptoms of a fractured skull.22

Artist: Jacob Jordaens
Vomiting Man, From The Bean King (1655)
Vomiting was another possible symptom of a damaging head wound according to John Moyle23, Richard Wiseman24, John Atkins25 and John Woodall26. Ambroise Paré suggested that if the patient "vomit choler [one of the four bodily fluids or humors, also referred to as yellow bile]" after a head wound, it was indicative of a fractured cranium.27 Woodall reiterated this point in his book, explaining that when other symptoms intensify and "a bilious or sharpe vomiting is seene" it indicates that the brain has been injured.28
Headaches and other pains in the head following a smashed skull could also be telling signs of a significant head wound. In one of Moyle's case studies he found that several days after a head wound "the Man complain’d of an exceeding great Pain in his Head: this Pain increasing so, that he had no rest Day nor Night. ...his Pain grew intolerable, especially under the place where the Blow was received; insomuch that I suspected there was a Fissure of the Cranium"29.
Pain in the head when biting something was a skull fracture symptom highlighted by two period surgical authors. John Moyle noted that he tested patients for such head wounds by
Artist: Frank Holl - Headache (1881)
putting a uvula spoon [a spoon-shaped instrument for holding the uvula down] in the patient's mouth, explaining that a symptom of a fractured braincase was that "he cannot hold it between his Teeth, without feeling extream pain in the part fractured; to which he will often lift his Hand."30 Fellow sea surgeon John Atkins noted a similar test for a patient which resulted in "a Pain [up]on biting any hard Body; and, perhaps, and often reaching of his Hand to the afflicted Part"31.
A few unusual suggestions for symptoms of a cracked cranium were also indicated. Paré suggested that "if his tongue be blacke with direnesse, if the edges of the wound bee blacke or dry, and cast forth no sanious matter, if they resemble the colour of salted flesh, if he have ...absolute suppression of the Urine and excrements" it was a dire sign of a skull fracture.32 John Woodall suggested that "hurt or ruption of the membranes or braine is accompanied with sneesing"33.
John Atkins concluded his discussion of symptoms on a practical note, explaining that "All, or some of these [symptoms] follow a Fracture immediately, and the Measure of a good or bad Prognostick is taken according to their Degree, and the Time of their Continuance."34 John Woodall explains that "sometimes there are dangerous symptoms that cease"35.
1 John Atkins, The Navy Surgeon, 1742, p. 76; 2 John Moyle, Memoirs: Of many Extraordinary Cures, 1708, p. 23; 3 Atkins, p. 76; 4 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p.204; 5 Richard Wiseman, Of Wounds, Severall Chirurgicall Treatises, 1676, p. 393; 6 Wiseman, p. 403; 7 John Woodall, the surgions mate, 1617, p. 126 (incorrectly paginated 134); 8 Moyle, Memoirs. p. 1; 9 Atkins, p. 76; 10 Atkins, p. 77; 11,12 Paré, p. 204; 13 John Moyle, The Sea Chirurgeon, 1693, p. 109; 14 Atkins, p. 77; 20 Moyle, Memoirs. p. 18; 16 Wiseman, p. 393; 17 Paré, p. 204; 18 Atkins, p. 76 & Woodall, p. 126 (incorrectly paginated 134); 19 Paré, p. 204; 20 Moyle, Sea Chirurgeon, p. 109; 21 Moyle, Memoirs. p. 1-2; 21 Atkins, p. 76; 23 Moyle, Sea Chirurgeon, p. 109; 24 Wiseman, p. 398 & 403; 25 Atkins, p. 76; 26 Woodall, p. 126 (incorrectly paginated 134); 27 Paré, p. 204; 28 Woodall, p. 126 (incorrectly paginated 134); 29 Moyle, Memoirs. p. 29; 31 Moyle, Sea Chirurgeon, p. 109; 31 Atkins, p. 76-7; 32 Paré, p. 204; 33 Woodall, p. 126 (incorrectly paginated 134); 34 Atkins, p. 76; 35 John Woodall, the surgions mate, 1639, p. 317
Aspects of Skull Wounds
A variety of different things impacted the severity of a skull wound which in turn suggested the treatment required.
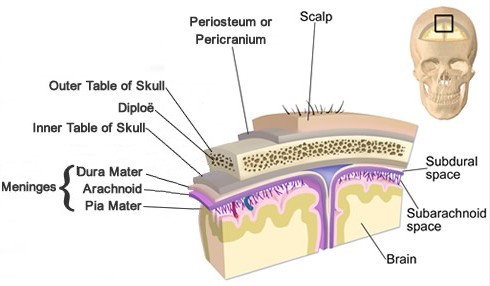
Image: Bruce Blaus, Modified by Mission
Layers Covering the Brain According to Surgeons in Late 17th/early 18th c.
(Note: The arachnoid
mater,
subarachnoid and subdural layers are more modern than the golden age of piracy.)
Not all skull wounds required procedures such as trepanning, elevation of the bone or rasping the edges of the skull. Sea surgeon John Woodall explained that it was "necessary for the wise Artist to know the manner of the hurt, that he may wisely prognosticate the danger" to the patient.1
Woodall explained that when "onely the Pericranium be hurt by incision, without any contusion [bruised tissue], and symptoms arise with a tumour in the head, then dilation [of the wound in the skin] is needefull [so] that the contused bloud which is between the Cranium and Pericranium may bee extracted, and let it be quickly done, so shall the symptomes cease and the cure will be easie"2.
Sea surgeon John Moyle likewise advised, "If you see not some of these signs [referring to the symptoms presented in the previous section], and yet see a Fissure [in the skull],

Artist: Jonas Arnold Delineavi
Head Surgery & Tools, From Armamentarium
Chirurgicum
Bipartitum,
Scultetus (1666)
you may conclude it to be but superficial, and only through the first Table, and there will be no occasion of Traphining [trepanning or making holes in the skull], but only Phlebotomy [blood-letting], and dressing the Head as in other Wounds thereof, Cures it."3 Moyle also noted that large fractures of the skull may not require trepanning because "there is room enough for the blood [caused by an intracranial haematoma] to issue out."4
Of course, many wounds were more serious and required more intense therapy. Woodall advised great care when the surgeon observed wounds of skull, where "the forme and magnitude thereof be well considered, observing also diligently what bone it is, and in what part it is hurt"5.
Slivers of bone posed a particular threat to the well-being of the patient. Moyle discussed cases where patients "had the Skull Fractured, so that there has been shivers [shards and slivers of bone] separated from the whole, and lying [pressing] in upon the dura mater."6 John Woodall counselled that in such fractured wounds of the skull "there is required great care ...whether the fragments are great or little, or sharp, pricking the Membranes or not, which of what sort soever they be they are diligently to be drawne out with as much ease as may be to the Patient, and if they cannot being broader within, then without, let the Trapan be carefully used"7.
Wounds that appeared small could pose large problems. Moyle mentioned men with "but a sleight Wound, or none at all (only Tumefaction [swelling]) and under it there has been a small Fracture or Fissure, but the Brain concussed, or shaked, or contused; and this latter Fracture is worse to Cure than the former [a large fracture], and of more dangerous consequence. For here the contused blood that lyeth within cannot come out, but must coagulate and putrifie, unless that means of the Traphine be used."8
The location of the wound was also important. Woodall explained that when "the offence of the Pericranium be in the [natural] suture of seame [of the skull] it is more dangerous, because the braine doth sympathize with it, if the Fibres passing through the sutures of the Pericranium from Dura mater be wounded or contused it exceeds the other in danger"9.
So there was much for the surgeon to consider about a wound. The greater his knowledge and experience was in dealing with wounds of the head, the better he would be able to deal with them.
1,2 John Woodall, the surgions mate, 1617, p. 134; 3 John Moyle, Sea Chirurgeon, 1693, p. 109; 4 Moyle, p. 107; 5,6 Moyle, p. 106; 7 Woodall, p. 135; 8 Moyle, p. 106; 9 Woodall, p. 134-5;
Head Surgery Page Menu: 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Next>>
Main Page • Tools & Procedures • Miscellanea • About the Author • Facebook Page
All original content copyright M. Kehoe • 2003-