

Treating Sprains and luxations Page Menu: 1 2 3 4 5 6 7 8 9 10 11 12 13 Next>>
Treating Sprains & Dislocations in the Golden Age of Piracy, Page 10
Specific Dislocation/Luxation Cure: Thigh or Hip
The thigh or hip is discussed by four of the five sea surgeons as well as French surgeon Ambroise Paré

Image: John Heilman - Superior (Outward) Hip Dislocation
and English surgeon Richard Wiseman. A thigh dislocation is always perfect, that is, it cannot partially dislocate, due to the structure of the ball on the femur and the socket in the pelvic bone. Sea surgeon John Moyle reports "This is the hardest to set of all bones, and requires the greatest strength (and not a little skill) to reduce it."1
Wiseman, Paré and sea surgeons John Atkins and James Handley all agree that the thigh can be dislocated four different ways: inward, outward, backward and forward. However, even Paré says it happens "most frequently inwards, next to that outwards, but very seldom either forwards or backwards."2 Nevertheless, he provides explanations for treating all four types of dislocation. Atkins and Handley suggest that the most common hip dislocation is inward. Atkins says that that seems to be the only possiblility3 while Handley notes that it happens "oftenest inwards, becaus there the edge of the Acetabulum [the place where the femur meets the pelvis] is lowest"4. This section will only look at the repair of thigh luxated inward and outward.
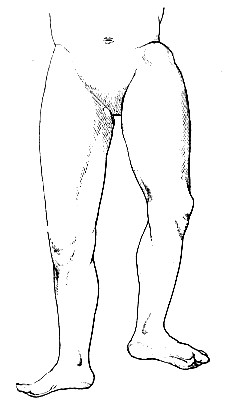
Outward Hip Dislocation, From Auteur de
l'Ouvrage, By Felix Marie Louis Lejars (1924)
The idea of a thigh being dislocated 'inward' or 'outward' is hard to picture. Fortunately, a description of the signs of these types of dislocation makes them a little clearer.
If the Luxation be inwards, that Thigh appears longer than the other, and the Knee, Leg and Foot stands outwards, and a Tumor appears near the Perinæum [the region between the back of the sex organs and the anus]. If the Luxation be outwards, the signs are the Contrary, that Leg is shorter; near the Perinæum there is an hollowness, the Knee, Leg, and Foot, stand inwards, and the Heel cannot touch the ground, nor deck.5
In addition to the above-mentioned signs, Paré adds that in these dislocations you can feel the head of the femur in the groin and the patient will not be able to bend his leg towards his groin.6 This description (combined with the X-Ray image above) sounds a bit counter-intuitive. Since the leg is long in an inward hip dislocation, the femur has come out of its socket and gone downwards - why not call it an downward dislocation? And why not call the outward dislocation an upward dislocation? However, the name appears to have only to do with the direction in which the bone left the socket, not what happened as a result. Once loosed from the hip socket, the muscles pull the femur in one direction or another resulting in the symptoms described.
Atkins notes that "the Violence which luxates the Hip, must prodigiously exceed that of any other" and will tear the ligament located at the base of the head of the femur. As a result, "the Pain and Influx of Humours will be proportionably aggested [heaped up]; and Inflammation, Apostemation [formation of pus], and perpetual Lameness, a more common Consequence of it."7 Wiseman agrees, suggesting that extension and reduction of the bone must be performed quickly to help prevent such complications.8
1 John Moyle, Chirugius Marinus: Or, The Sea Chirurgeon, 1693, p. 123; 2 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 389 (mispaginated); 3 John Atkins, The Navy Surgeon, 1742, p. 107; 4 James Handley, Colloquia Chyrurgica, 1705, p. 159; 5 Handley, p. 159-60; 6 Paré, p. 389 (mispaginated); 7 Atkins, p. 108; 8 Richard Wiseman, Severall Chirurgicall Treatises, 2nd ed., 1686, p. 495
Extending and Replacing a Dislocated Thigh/Hip
The surgical authors under study mention six ways to extend and replace a luxated thigh: three of them are simple, using only hands a belts, and the other three use devices. Let's look at each.
Extending and Replacing a Dislocated Thigh/Hip: Simple Methods
The three simple ways for extending and replacing a luxated thigh include: 1. A Single Person Extending the Dislocated Hip, 2. Multiple People Extending the Dislocated Hip and 3. Using a Ligature to Extend the Dislocated Hip.
1. A Single Person Extending the Dislocated Hip
Sea surgeons James Handley and military surgeon Richard Wiseman both discuss having one person extend a hip dislocated inward. Both note that this can be used when the patient is young with Handley adding that it can also be used when the dislocation is new. Handley describes it quickly: "it may be reduced with small Extension, and then suddenly to bend the Thigh."1 Wiseman is a little more expansive. He says the surgeon "must lay one Hand upon the Thigh, and the other upon the Patient's Leg; and having somewhat extended it towards the sound Leg, he must suddenly force the Knee up towards the Belly, and press back the bead of the Femur into its Acetabulum [hip socket], and it will knap in."2 He adds that such a dislocation is not a 'great' extension which is part of the reason this works.
2. Multiple People Extending the Dislocated Hip
Handley and sea surgeon John Atkins each discuss extending an inward dislocated thigh using three people. Handley's explanation is characteristically brief: "Let an

Multiple People Extending the Thigh with Ligatures, From Armementum Chirurgicum,
By
Johannes Scultetus, p. 114 (1666)
Assistant hold the Patient fast by the Arm-pits, and another take hold of the Thigh above the Knee, with both his Hands, and make Extension, then do you with your Hands force in the Bone."3
Atkins' explanation is also quite short, although it is a different than Handley's. He recommends placing a person between the patient's legs with a "strong Grasp about his [the patient's] Body, [to] hinder his receding or giving way, which is the Contra-Extention... while the Surgeon with both Hands above the Knee, extends forward, (an Assistant bearing the Foot up,) and at the same Time carries it towards the sound Thigh, and upwards"4. Because extension of an inwardly dislocated thigh didn't require 'great Extension' as Wiseman put it, this method could work.
3. Using a Ligature to Extend the Dislocated Hip
John Atkins and Ambroise Paré both use ligatures or bands to reduce a dislocated thigh. Although this is technically a device, it is treated here like a simple one as it was in the discussion on dislocated shoulders.
Atkins uses them as part of his discussion on having multiple people extend a hip dislocated inwards. If the surgeon didn't have a man strong enough to stand between the patient's legs and keep him from moving, he could instead have two assistants employ "a strong Towel [placed] up the Twist [the hollow on the inside of the thigh]"5 to keep the patient steady during relocation of their hip.
Paré recommends a ligature for both an inwardly and outwardly dislocated thigh. For an inward dislocation, he suggests a "ligature shall bee put upon the joint directly at the hip, &
 1649.jpg)
Multiple People Extending the Thigh with Ligatures and a Pulley, From The Workes of
that
Famous Chirurgion
Ambrose
Parey, p. 394 (1649)
held stiff by the hands of a strong man, yet so that it may not touch the head of the thigh by
pressing it, for so it would hinder the restoring thereof."6 Using this force, the muscles "may give way and yeeld themselves more pliant, then must the rope bee somwhat slacked, and then you must also desist from extending, otherwise the restitution cannot bee performed, for that the stronger extension of the engine will resist the hand of the Surgeon"7.
The procedure for an outwardly dislocated thigh was a little different. "The patient must bee placed groveling [face down] upon a table ...and ligatures as before, cast upon the hip and lower part of the thigh, then extension must be made downwards, and counter-extension upwards; then presently the head of the bone must bee forced by the hand of the Surgeon into its place."8 Paré says that if this didn't work, his pulley would be needed for the extension which is what he shows being used in his book.
Extending and Replacing a Dislocated Thigh/Hip: Complex Methods
There were three complex methods suggested for relocating a dislocated hip bone, all of which used devices to extend the femur. These include: 1. Extending a Dislocated Hip Using a Pin, 2. Extending a Dislocated Hip Using a Pulley and 3. Extending a Dislocated Hip Using the Commander.
1. Extending a Dislocated Hip Using a Pin
This is by far the most popular method for repairing a dislocated thigh. It is mentioned by all of the surgeons who discuss this type of dislocation. Sea surgeon John Moyle provides a fairly good description of how a pin is used to treat an inward dislocation of the hip.
Drive a strong Trummel of Wood, or long Bolt of Iron into the Deck; or long Bolt of Iron into the Deck; then lay the Patient on his Back, with this bolt between the Legs; let there be a hard bolster likewise in his Groin, on the head of the dislocated bone, and the bolt close up to that.
Then make fast the Leg on the contrary side, and likewise the Thigh, that the Man may not give way when the other is extended; and let his Body be kept steady also, that he may not incline his Body.9

Photo: Mission - The Peg
The other four authors who discuss inward thigh dislocations follow this procedure. Atkins first suggests using the hands only on an inward hip dislocation, resorting to ligatures only if that is inadequate.10
Handley, also writing for an inward dislocation, provides some interesting details about the peg/pin. He recommends using "a Wooden Pin ...drove into the Floor or Deck... with this Pin between his [the patient's] Legs, placed close up to the head of the Bone, with a thick hard boulster between them"11. Paré's description mentions the pin should be "of a foot’s length, and as thick as the handle of a spade useth to be; but it must be wrapped about with som soft cloth, lest the hardness hurt the buttocks, betwixt which it must stand"12.
In addition to the pin keeping the patient from sliding downwards, Paré notes that "there is no great need of counter-extension towards the upper parts [because the pin serves this function]; and besides it helpeth to force back the bone into its cavitie, the help of the Surgeon concurring, who twining somwhiles to this, & otherwhiles to that side, doth direct the whole work."13 The pin is here basically serving a purpose similar to that which the knob on the end of the ambi serves in a shoulder luxation.
Richard Wiseman also recommends using a pin in an outward dislocation, explaining that the patient is to be placed face down just like Paré recommended in his description of outward dislocation using ligatures. He explains that in this case "the Pin [is] placed as aforesaid in his Twist it ought to be as thick as a Rowling-pin, and covered with Cotton, that its hardness may not be offensive. The Extension may also be made upward by a Towel or Girt between his Thighs"14.
2. Extending a Dislocated Hip Using a Pulley
The pulley is always combined with other methods when used for thigh dislocations. Paré's recommendation for its use with ligatures in an outward hip dislocation has already been mentioned. Richard Wiseman also mentions using a pulley in treating an outward hip dislocation.
 1649.jpg)
Using a Pulley to Extend the Thigh, From The Workes of
that
Famous Chirurgion
Ambrose
Parey, p. 393 (1649)
"The Extension may also be made upward by a Towel or Girt between his Thighs: and the while that Leg must be stretcht by Pulleys or such like strength, and the Bandage [to which the pulley is attached] fastened above the Knee."15
The pulley and pin were used together as well. Sea surgeon Moyle advised the surgeon that after he had situated the patient on the pin to "have a Pully made fast at a distance, with a Pully-rope, having a hook at the end of it; make fast that is dislocated. Then let a strong Man haul forcibly and suddenly at the other end of the Pully-rope, and your Hands guiding about the Joynt, and by this means the bone will fly into its place."16 Handley similarly uses a pulley with the pin, telling the surgeon to "apply a strong soft Rowler several times about his dislocated Thigh, to which a Cord or Pully must be fixed, with its other end at some distance, then an assistant must haul strongly upon the Cord, [and] make Extension"17.
Atkins suggests the use of a pulley instead of the pin to extend the thigh for an inwardly dislocated thigh, but doesn't provide much detail, only noting that it thrusts "the Thigh backwards and outwards at the same Time."18
3. Extending a Dislocated Hip Using the Commander
The commander is used by sea surgeon John Woodall, who is tireless in promoting it for extending dislocations, although he doesn't specify whether it could be applied to inward or outward dislocations. Given its function, it could presumably be used on both. Woodall does give specific instructions when using the commander on a dislocated thigh. In this application,
the button [also called the ball, which is used in dislocations of the shoulder] on the top must be taken off, and a cushion bound on the place thereof; the party must also be so placed lying that his huckle [hip] bone, thigh and legge must hange over the beddes feet from the bedde, or so laid on a table that all those parts may bee free, and his legge below the knee must be gently bound to the Commander19
Without fully understanding the design of the Woodall's commander, it's difficult be sure how this worked. However, the cushion is basically serving the same role as the pin does, pushing against the patient's pubic bone and possibly then pushing up the head of the femur as well. The end of the commander tied to the knee is meant to pull it down against the pubic bone and so extend the thigh.
1 James Handley, Colloquia Chyrurgica, 1705, p. 160; 2 Richard Wiseman, Severall Chirurgicall Treatises, 2nd ed., 1686, p. 495; 3 Handley, p. 160; 4 John Atkins, The Navy Surgeon, 1742, p. 108; 6 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 392-3 (mispaginated); 7 Paré, p. 393; 8 Paré, p. 393-4; 9 John Moyle, Chirugius Marinus: Or, The Sea Chirurgeon, 1693, p. 123-4; 10 Atkins, p. 108; 11 Handley, p. 160; 12,13 Paré, p. 392 (mispaginated); 14,15 Wiseman, p. 495; 16 Moyle, p. 124; 17 Handley, p. 160-1; 18 Atkins, p. 108; 19 John Woodall, the surgions mate, 1639, p. 156
Securing a Dislocated Hip and Post-Operative Care
As with most of the later descriptions of medicines for luxations in their books, the surgeons are brief in describing what medicines should be applied to a repaired hip dislocation. Richard Wiseman again suggests restrictives, designed to protect the area from air and unwanted humors.1 Sea surgeon John Moyle tells his readers to , "embrocate with warm Ol. Rosarum [oil of roses],
Dressing the Thigh, From L' Arecenal de Chirurgery,
By
Johannes Scultetus, frontispiece (1672)
and apply the defensive Plaster [such as his own defensivum minor]"2. Ambroise Paré also stays true to form, recommending agglutinative medicines3. When discussing the bandage to be applied, Charles Gabriel Le Clerc suggests that the compress be "wetted in Oxycrate [water and vinegar] or Wine heated, to encompass the Joint"4.
Sea surgeon John Atkins gives a recommendation similar to Le Clerc's, but he adds some very interesting comments about the purpose of the medicines here.
I should think a Compress dipped in Oxycrate, or Red Wine, large enough to infold the whole Joint, and crossing upon the Hip, would be better than Emplaisters, which obstruct the Perspiration of the Part, and by that means raise a Ferment in the Humours, more rationally supposed to be aggregated, where the Hurt and Extention to restore it have been both so very great.5
This really highlights the role of the humors in wounds. As noted previously, sweating was believed to be a way for the body to eject unwanted humors. Atkins is saying that not allowing a repaired hip luxation to sweat stirs up (ferments) the humors which then combine together (aggregate) at the wound site.
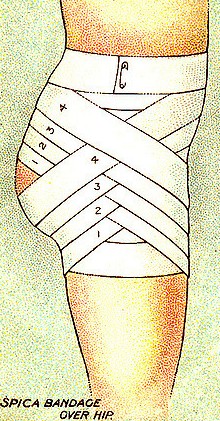
Spica Dressing On the Hip, From Will's
Cigarettes First Aid Card (1913)
For bandaging, Atkins says to use a roller bandage that is "long and double, and like the Compress, cross over the affected Hip, and so continue with Crosses and Edgings till finished."6 Sea surgeon John Woodall simply advises the surgeon to provide "neat ligature"7 and Wiseman orders "good Compress and Bandage"8, probably to prevent discomfort when lying on it. Both Wiseman and Paré recommend binding the patient's legs together. Paré specifies that this be done when the dislocation is accompanied by a fracture "whereby the dislocated member may be unmoovable, and more & more strengthned."9
Paré offers some detailed information on applying the dressing. He says the bandaging (using a roller bandage apparently) should start at "the place whereinto the head of the thigh fell, and thence brought to the opposite or sound side by the belly and loins. In the mean while the cavitie of the groin must bee filled with somwhat a thick bolster which may keep the head of the bone in the cavitie."10 After that, it is to have 'junks' applied to it. These are pieces of cloth rolled with stiff, grass-like plants inside them which were to serve as soft splints. They were applied from the top of the hip to below the ankle. Paré ordered that the dressing be kept tightly on for four or five days unless some complication occurs which made its removal necessary.
French surgeon Le Clerc suggests a different kind of dressing, a variation on his spica which he also used for dressing dislocations of the shoulder and fingers. The bandage was to be two inches wide and about a hundred inches long. It began on the hip opposite the one that was dislocated and then was wrapped across the dislocated hip. It was crossed and re-crossed creating an X pattern on the wounded hip as seen in the image above. "You must not make any Spica on the sound Hip, but only Rounds, that is, you pass the Turns of the Roller one over another, without leaving any Edging either on that Hip, or the Belly, or behind the Back, but only on the part affected. Fasten the remaining Pan of your Roller by Rounds about the Body, and so pin it."11
Bed Rest, From L' Arecenal de Chirurgery,
By
Johannes Scultetus, p. 59 (1665)
For long term care, bed rest was the order of the day. It is the first recommendation Wiseman makes.12 Atkins similarly suggests the patient be left "resting the Hip on a soft Pillow, with the Knee and Foot a little raised, and continued for three Weeks in the quietest and easiest Position."13 Paré says the patient is to stay in bed for a month so that "the relaxed muscles, nervs and ligaments may have space to recover their former strength, otherwise, there is danger left the bone may again fall out by the too forward and speedy walking upon it."14
Atkins and Moyle both advise letting blood and dieting with Moyle specifying vulnerary or healing drinks.15 Atkins includes clysters (enemas) to his recommendations, explaining that such things "contribute likewise their Share in preventing Fever and other Disturbances."16 Although he doesn't spell it out, the complications were believed to arise from the generation and concentration of unwanted humors resulting from the wounded hip.
In a somewhat related tone, Wiseman adds that if the femur is believed to have fallen because the joint was relaxed because an excess of humors made it softer and more slippery, "good drying and corroborating Fomentations, Emplasters, Epispasticks [blister plasters], Fontanels, &c" must be administered.17
1 Richard Wiseman, Severall Chirurgicall Treatises, 2nd ed., 1686, p. 495; 2 John Moyle, Chirugius Marinus: Or, The Sea Chirurgeon, 1693, p. 123-4; 3 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 393 (mispaginated); 4 Charles Gabriel Le Clerc, A Description of Bandages and Dressings, p. 73; 5,6 John Atkins, The Navy Surgeon, 1742, p. 108; 7 John Woodall, the surgions mate, 1617, p. 156; 9,10 Paré, p. 393 (mispaginated); 11 Le Clerc, p. 73-4; 12 Wiseman, p. 495; 13 Atkins, p. 109; 14 Paré, p. 393 (mispaginated); 15 Moyle,, p. 124 & Atkins, p. 109; 16 Atkins, p. 109; 17 Wiseman, p. 495
Treating Sprains and luxations Page Menu: 1 2 3 4 5 6 7 8 9 10 11 12 13 Next>>
Main Page • Tools & Procedures • Miscellanea • About the Author • Facebook Page
All original content copyright M. Kehoe • 2003-