

Treating Sprains and luxations Page Menu: 1 2 3 4 5 6 7 8 9 10 11 12 13 Next>>
Treating Sprains & Dislocations in the Golden Age of Piracy, Page 5
Specific Dislocation/Luxation Cure
This brings us to the cure of particular dislocations. The methods for treating luxations were largely specific
A Primative Leg Extension, From Vidi Vidii Opera varia, By Galen (1599)
to the particular bone that was out of place and sometimes even to the way in which it had been dislocated. However, the four intentions of the general cure of dislocations/luxations discussed previously was used as a way to outline the cure of each particular dislocation. For review, the four intentions or steps for repairing a dislocated/luxated joint are:
1. Extend the Dislocated Joint/Bone
2. Replace the Dislocated Bone
3. Secure the Repaired Dislocation
4. Administer Post-Operative Care
With these in mind, the steps will be used here to organize the explanation of each type of dislocation. Since replacement occurred almost simultaneously with extension they are combined in the same sub-section; trying to separate them would make the explanations confusing. Securing the part through medicine and bandage and post-operative care are usually only briefly described, so they will also be placed together in their own subsection. When explanations are particularly brief, all the steps are combined into a single section.
A number of types of dislocation are discussed by the seven surgical authors whose texts are used in this part of the article. Among them, French surgeon Ambroise Paré gives the most complete review. However, Paré's book was written for the general surgical audience and includes several things that would not have been of interest to many sea surgeons. For example, Paré gives detailed cures for luxations of the head, toes and palm of the hand, something the five sea surgeons whose books are used here didn't do. This is probably because they were unlikely to occur on a ship. With this in mind, this article discusses only those luxations mentioned in the sea surgeon's books.
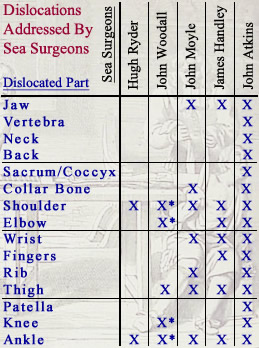
Dislocations Addressed by Sea Surgeons.
* Indicates
that the author
only mentions this type.
Image:
Armentarium Chirurgicae, Sculeteus (1693)
The list of the dislocations each of the sea surgeons talk about can be seen at left. The first notable thing about this list is that John Atkins discusses every type of dislocation mentioned in a sea surgeon's book from this period. His is the most complete and detailed compilation of luxation cures among the sea surgeons.
Atkins notes that some bones have an 'obscure motion' and, as a result, they "seldom luxate; but when they do, are most difficult of Recovery."1 These include dislocations of the spine (including the neck, back and sacrum/coccyx), the ribs and the patella (which he calls the rotella). Unlike the other dislocations in the list, Atkins does not give them individual sections in his book nor does he provide lengthy description of their cure. This suggests they were uncommon and unlikely to be read by a naval surgeon who was hurriedly flipping through his book looking for a particular cure.
Only five luxations are discussed by more than two sea surgeons: the shoulder, elbow, wrist, thigh and ankle. Based on this, it is likely these would have been the most common types of dislocations a sea surgeon faced.
Sea surgeons John Woodall and Hugh Ryder do not actually break the cure of dislocations out into individual sections at all, so their contributions to the particular cures are rather limited. John Moyle, James Handley and Atkins all give common dislocations individual sections for easy reference. Handley's book is written in a Question and Answer fashion that actually makes information very easy to find. His and Moyle's books are probably the best general survey of the types of dislocations a sea surgeon would encounter in his career at sea. Unlike Atkins book, which explains the workings of the bones and muscles before explaining the cure of each dislocation, Moyle and Handley skip most of the theory and proceed to the cure - something that would likely have been appreciated by a sea surgeon working on a variety of different cases in the dim recesses of his ship.
1 John Atkins, The Navy Surgeon, 1742, p. 97
Specific Dislocation/Luxation Cure: The Jaw
The jaw can be dislocated in a variety of ways. These include "Any thing that over-stretcheth the Mouth, whether yawning, gaping or chewing"1 as well as "weakness, sickness, cold or sleepiness"2. Sleepiness may indirectly refer to the need to yawn.
Most of the surgical authors agree that jaw dislocation can occur either on one or both sides, although sea surgeon John Atkins points out that "Stress can very rarely [be brought to] bear upon both Sides [of the jaw] at the same time. When it does, the Luxation is
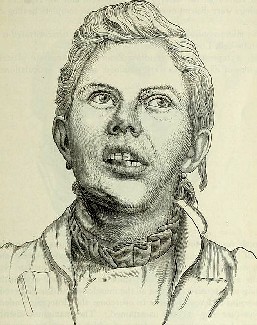
Patient With a Jaw Dislocated on His Left Side,
From The Dental cosmos, By J. White (1891)
perfect, several ingenious Surgeon have laid it down as mortal."3 Atkins' opinions about its deadliness notwithstanding, a treatment for a perfect (double) dislocated jaw is presented which will be discussed here.
Most surgeons concur that the jaw can be luxated forward - that is, it can only be unseated from its joint away from the body. However, the opposite is not true. Richard Wiseman states that the only way the jaw could be dislocated towards the body is if it were fractured.4 Ever thorough, French surgeon Ambroise Paré confesses that he has never seen the jaw unseated backwards, but still presents a method for fixing it.5
The signs of a dislocated jaw are "the lower Jaw is thrust forward, the Teeth are prominent beyond those of the upper, the Patient can neither swallow nor speak nor chew, nor indeed shut his Chaps [chops]... the fore-part of the Jaw is thrust down on one side, &c."6 Paré adds that "the place is hollow from whence it [the jaw] is flown, but swoln whither it is gone"7. He also describes a double luxation of the jaw, explaining that "all the jaw and chin hang forwards and towards the breast; besides also, the temporall muscles appear distended, spittle runs out of the Patients mouth against his will, the lower teeth stand further forward than the upper"8. He says the patient cannot speak, but only stammers.
Several of the surgeons mention that if the dislocation happened several days ago, there may be a tumor and there will be tightness in the muscles. Paré tells his reader that if this is the case, "before you go about to restore it, you must use softning and relaxing medicins to it"9. He does not specify which medicines are to be used.
Extending and Replacing a Dislocated Jaw
Replacing a jaw dislocated on one side begins with the proper position of the patient. "In order to the Reposition of the Jaws, the Patient ought to be seated firm, and his Head held steady, lest it start back in the time of Reduction."10 Paré recommends the patient "be placed on a low seat, so that he may be under the Surgeon;
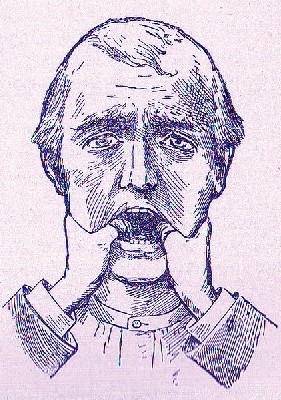
Fixing a Dislocated Jaw, From Points in Nursing,
By Emily A. M, Stoney (1910)
then [with] your servant, standing at his back."11 He also says that the patient, in "as much as in him lyes, shall help forwards [advance] the Surgeons endeavor, in opening his mouth as little as he can, lest the muscles should be extended; and he shall only gape so wide as to admit the Surgeons thumb"12. Wiseman advises using wooden blocks to keep the mouth open during the operation, placed "close between his great Teeth, as far as you can thrust them, and your Thumbs close by them, and your Fingers externally under both the Jaws"13. Both he and Paré recommend that the surgeon wrap his thumbs in folded linen or similar cloth both to protect them from the patient's teeth and to keep them from slipping while pressing down on the jaw. Paré warns not to have the patient open his mouth too wide, or the temporal muscles "will be extended after a convulsive manner" and work against the relocation of the jaw.14
With the patient thus positioned and the surgeon having his thumbs on the patient's lower molars, Paré, Wiseman and John Atkins all recommend the same basic procedure: "with your Thumb ...pressing that part downwards, ...raise the fore-part upwards by a quick moderate Extension, and you shall feel it reduced [go back into place]"15. Atkins notes that once the jaw is reduced, "it may be heard to snap in."16 If the dislocation has been properly restored, Wiseman explains that the surgeon "may conclude it so by the equal meeting of his [the patient's] Teeth and by the opening and shutting or his Mouth, also by his ready Speech."17
Both sea surgeons Atkins and John Moyle suggest alternative ways of performing this operation. Atkins' method is simplest, noting, "Those who do not care for Ceremony, use a Slap of the Chops, on the Side contrary to the Luxation."18
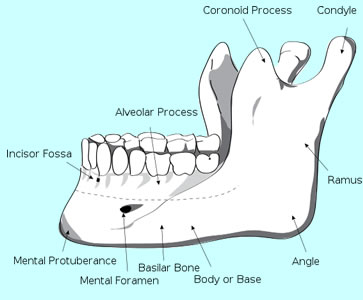
Artist: Djexplo - Labeled Human Mandible (Jaw)
Moyle's method is a little more elegant. He advises his readers to "Put your finger into the Patients Mouth, and you will feel a Bump [referring to the condyle of the jaw] towards the place of the Joynt; which bump is the head of the Bone out of place."19 Once the condyle is located, Moyle says to "put your Thumb within the Mouth to that bump, and the palm of your hand at the Chin without, and the other hand behind his head to hold him to you. Then thrust back with your Thumb, and the Chin with your hand, and the bone will fly into its place."20 Note that both Atkins' alternative and Moyle's method are simple and straightforward, not requiring assistants. Sea surgeons on smaller vessels sometimes found themselves without help, which may explain this.
Paré is the only author to discuss a method for repairing the jaw when both joints are luxated. The preparation is not much different than for a single jaw luxation, except that he suggests the patient may be placed on the ground. The surgeon to put his thumbs on the patient's molars, wrapped in cloth and put his fingers under the patient's chin so he can lift it up. The primary difference in technique involves what the surgeon should do if the patient cannot open his mouth. Paré says
then must you thrust in woodden wedges made of soft wood, as hazle, or firre [pine], being cut square, and of some fingers thick ness. These shall be wedged in on each side above the grinders [molars]; then cast a ligature [strip of cloth or soft rope] under his chin, whose ends your servant shal hold in his hands, and setting his knees upon the Patients shoulders, shall pull them upwards; then at the same time the Surgeon shall press downwards the woodden wedges.21
From this description, It becomes clear why the patient might want to be seated on the floor.
Securing the Relocated Jaw and Post-Operative Care
Once the jaw was in place the next step was to medicate and bandage it. For topical medicines, John Moyle advises either the use of Unguent. Martiatum (soldier's ointment) or hot oil.22 Paré suggests "a medicine made of the whites of egs, and oil of roses to asswage pain, and apply cloths dipped in oxycrate [water and vinegar]."23 For pain, Wiseman recommends that the surgeon "embrocate the Temporal Muscles and Parts about with ol. lumbricor. [oil of earthworms] mastichin. [oil of mastic tree resin] &c."24 He also says that if the surgeon fears the joint will prolapse he can apply a defensative (a medicated plaster designed to keep the air from getting to the wound), although he adds that "hitherto I never saw occasion to apply any thing."25 James Handley adds "if need be, apply astringents [medicines to contract tissues] also"26.
Single Side Jaw Luxation Dressings, A
Description of Bandages and Dressings,
By Charles Gabriel Le Clerc (1701)
Most of the surgeons don't say much about bandaging this sort of wound. Moyle alone recommends that his reader "wrap a piece of Flannel about the Jaws, and give him {1 dram} of Venice Treacle [a sort of cure all during this period] in a little burnt Wine."27 The flannel was likely to keep the jaws held shut, something recommended by several of the surgeons.
Charles Gabriel Le Clerc suggests bandages for both a single and double jaw luxation in his book on bandages. Since the bandages for both types of dislocation are similar, we will look only at his recommendation for the single dislocation of the jaw. For reference, Le Clerc includes diagrams of his dressings with strings connecting the various components as seen at left. (The string is not related to the bandage.)
The first two element of Le Clerc's bandaging system are dressings. The first (at the bottom of the image, with a 1 on it) is a compress, most likely made of soft linen, folded over several times in the rough shape of the jaw. "Before it be applied, it must be dipt in Oxycrate or Red-wine, warmed to strengthen the Part, and prevent Fluxion [flows - referring to flows of humors within the joint]."28 Next (2) is a piece of pasteboard made in the same configuration. Paste boards are thin firm boards made from sheets of paper pasted together. They are similar to the material found on the inside of a hardbound book cover. The pasteboard piece is used as a splint to hold the jaw in place after it has been re-seated.
The last element (4) is a roller bandage, likely of linen or some similar soft material, about three inches wide and an ell (roughly 18 inches) long with each end split so that it has four 'tails'. It has a diamond cut out in the center for the chin to go through. Le Clerc explains that once the patient's chin has been put through the diamond, the surgeon is to "bring the upper Tails over the top of the Head, a little backwards, and cross them, then bring back the ends over the Temples, or on each side, and pin their Extremities:

Artist: J. Bell - Mandible Bandage, Although
Different
Than Le Clerc's
(18th century)
Take the two lower Tails and cross them, ascending over the upper, pass them over the top of the Head, and cross them, then bring back the ends to the Temples, and pin them to the Patient's Cap."29 Like Moyle's simple piece of flannel, this bandage is basically designed to keep the jaw shut.
A few post operative-care notes are given for finishing the cure. Paré tells the surgeon to "forbid the Patient to speak, or needlesly open his mouth. Wherefore he must abstain from hard meats [hard foods], and such as require much chewing, untill his pain be quite passed, and use only spoon meats [soft foods], as Barley-creams, ponadoes [panadas - gruels with a base of bread crumbs, toast, flour or other grains], jellies, cullassas [probably calases - fried dumplings], broths, and the like."30 Handley similarly recommends that "for three or four Days keep him [the patient] to Liquids only."31 This is all to keep the patient from moving their jaw so that it doesn't prolapse.
Moyle advises that the surgeon put the patient "in a breathing Sweat, and he will be well presently and not yawn at all."32 A breathing sweat is a fairly low intensity sweat typically induced by extra clothing, warm rooms or medicines. Its intent was to purge unwanted humors from the body. In a similar effort to draw off unwanted humors, Handley recommends bleeding the patient.33
Paré suggests some additional medicines for the second dressing. (Keep in mind that it was generally recommended that the first dressing of a dislocated joint be left on for several days.) He uses topical medicines which are "to agglutinate ['glue'] and strengthen the ligaments and other relaxed parts, and also to keep it being restored in its place."34 He then recommends a medicine which is a slight variation on that he advised in his discussion of the general cure of dislocations (found here). "[A]fterwards you may use emplast. Diacaleitheos dissolved in oil of roses and vinegar, and other things, as occasion shall be."35
1 John Atkins, The Navy Surgeon, 1742, p. 102; 2 John Moyle, Chirugius Marinus: Or, The Sea Chirurgeon, 1693, p. 103; 3 Atkins, p. 102; 4 Richard Wiseman, Severall Chirurgicall Treatises, 2nd ed., 1686, p. 482-3; 5 This will not be included here. For those interested, see Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 384; 6 Wiseman, p. 483; 7,8,9 Paré, p. 383; 10 Wiseman, p. 483; 11 Paré, p. 383; 12 Paré, p. 384; 13 Wiseman, p. 483; 14 Paré, p. 384; 15 Wiseman, p. 483; 16 Atkins, p. 102; 17 Wiseman, p. 483; 18 Atkins, p. 102; 19,20 Moyle, p. 104; 21 Paré, p. 384; 22 Moyle, p. 104; 23 Paré, p. 384; 24,25 Wiseman, p. 483; 26 James Handley, Colloquia Chyrurgica, 1705, p. 155; 27 Moyle, p. 104; 28,29 Charles Gabriel Le Clerc, A Description of Bandages and Dressings, p. 17; 30 Paré, p. 384; 31 Handley, p. 155; 32 Moyle, p. 104; 33 Handley, p. 155; 34,35 Paré, p. 384
Treating Sprains and luxations Page Menu: 1 2 3 4 5 6 7 8 9 10 11 12 13 Next>>
Main Page • Tools & Procedures • Miscellanea • About the Author • Facebook Page
All original content copyright M. Kehoe • 2003-